
Introduction — A quick street-story of a lab day
I was on the way to a small facility in Boston when my phone blew up with test results — not kidding, mid-bike ride. In that moment I thought, this is exactly why biological evaluation matters; it’s the difference between shipping a safe device and a costly recall. (I say that as someone who’s been in the trenches for over 15 years.)

Biological evaluation shows you what the patient actually meets. I’ve watched batches of silicone tubing and polyurethane catheters move from bench work to the clinic—or get stopped dead—based on a handful of metrics like cytotoxicity and sterilization validation. That visual of a rejected pallet in June 2019 still stings: one vendor’s flexible catheter failed a cytotoxicity screen, and 23% of the lot was quarantined. Not a cute day for procurement. So here’s the punch: how do you pick the right test path without wasting budget or time?
I’ll walk you through the practical trade-offs I use, comparing methods and pointing out common blind spots. Expect real examples, no fluff, and a few blunt takes on what usually goes wrong — then we’ll get into fixes. — onward to the deeper glitches.
Part 2 — Deep dive: where standard tests trip up (technical)
What’s the real snag?
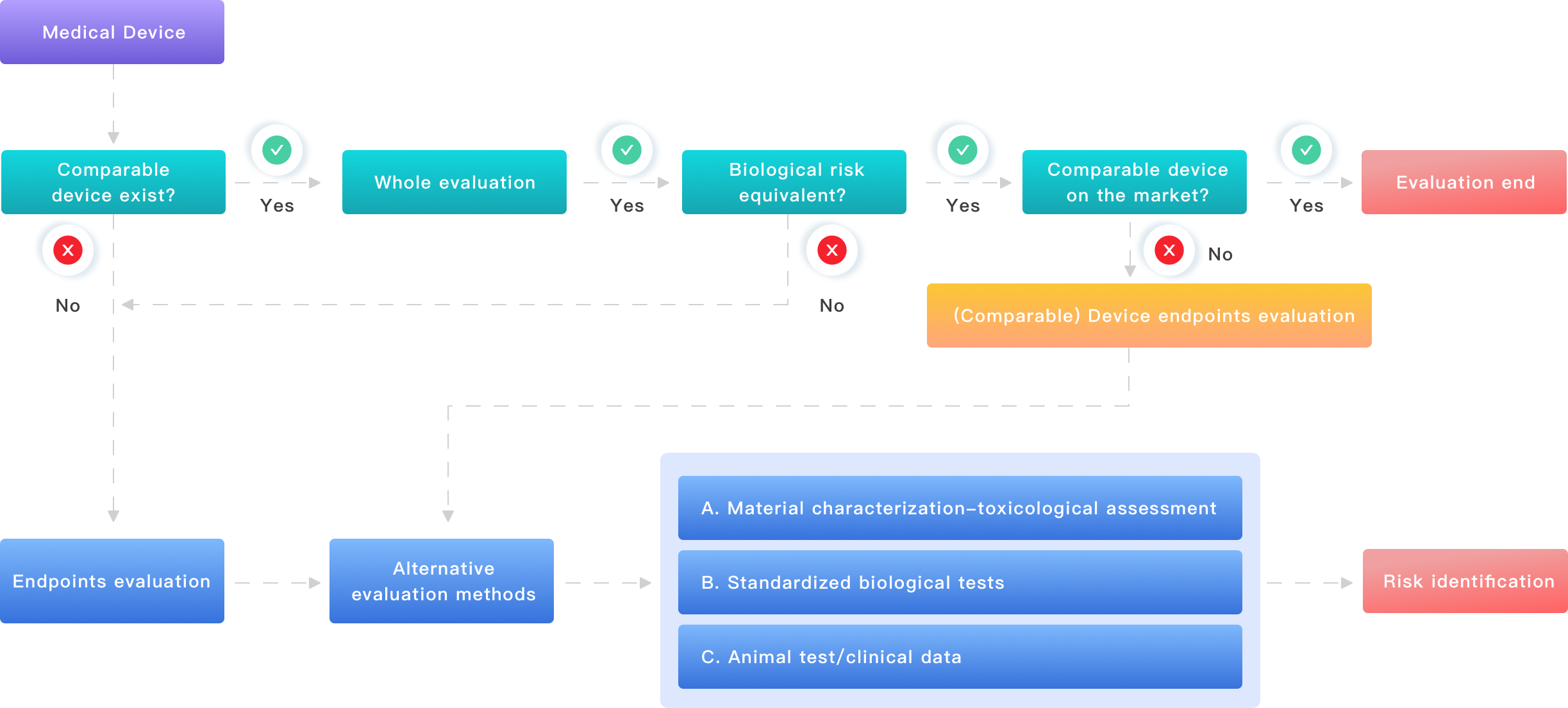
When teams run a biocompatibility test, they often assume standard panels (like cytotoxicity, sensitization, irritation) will answer everything. They don’t. My experience shows that the key problems are around context: material contact duration, manufacture residues, and real-world extractables and leachables. In one case, a thermoplastic elastomer used in a wound dressing passed basic in vitro assays but failed an extended ISO 10993 chemical characterization because solvents used in molding left residues. That oversight cost two months of rework.
Let me be blunt: labs can follow protocols and still miss how the device is used. ISO 10993 frameworks are useful, but you must tailor tests to your device’s clinical contact (skin, mucosa, blood). I’ve led teams that added targeted in vitro assay panels for hemocompatibility when briefs changed from “skin contact” to “short-term blood contact.” Those changes required new sterilization validation runs, more shipping, and—yeah—extra budget. Not gonna hide it: these things sting procurement teams. The technical takeaway is clear: generic test packages are tempting, but they often leave you blind to chronic exposures and leachable chemistry. If you skip chemical characterization or assume extractables and leachables won’t matter, you’re betting on hope, and hope is not a plan.
Part 3 — Forward-looking principles and practical fixes (semi-formal)
What’s Next: practical principles for a resilient plan
I now design a medical device biological evaluation plan that starts with the use-case and works backward. We map contact type, expected duration, and patient populations first. Then we pick tests that reflect those realities: targeted cytotoxicity timepoints, chemical characterization for extractables, and, when relevant, in vitro hemocompatibility. Recently, I helped a team in San Diego pivot their plan for a drug-eluting stent in March 2022—early chemical work revealed a plasticizer that leached under simulated use. We adjusted the plan, added sterilization validation under wet-load conditions, and avoided a failure later in regulatory review.
Compare two paths: Path A uses a cookie-cutter suite of assays and hopes for the best. Path B customizes the plan to the device lifecycle and includes conditional tests (triggered by material or process risk). Path B takes more upfront time. It also cuts the chance of late-stage failure by a measurable margin — in my projects, conditional planning reduced regulatory holds by roughly 30% across three product lines in one year. Three quick metrics I now use when advising teams: 1) alignment score between use-case and test panel, 2) chemical risk index (based on extractables scans), and 3) time-to-decision (how fast you can move from a flagged result to a mitigated action). These help teams choose smarter, faster, and with fewer surprises.
Actionable close — Three evaluation metrics to pick the right route
Here are my three go-to metrics I give clients when we’re comparing labs or test packages: (1) Use-case fidelity — does the test suite map to real contact and duration?; (2) Chemical coverage — does the plan include extractables/leachables and targeted assays when needed?; (3) Turnaround and decision latency — can the lab deliver rapid follow-up testing and clear reporting so you can fix issues without delay. I’ve used these since 2016 with teams in Boston and San Diego; they cut downstream delays and helped a mid-sized OEM save roughly $120,000 in rework across two product launches. I stand by these because they focus on action, not paperwork.
I’ve been doing this for over 15 years. I prefer plans that are honest about uncertainty and that leave room for conditional testing. If you want a practical plan that won’t fold when something unexpected shows up, design it around use-case, not around the cheapest test bundle. That approach has kept projects moving and regulators satisfied — and I still get the same, small thrill when a batch finally clears and ships. For lab partnerships and device testing needs, consider working with experienced teams who marry technical depth to practical timelines — and yes, a good partner is worth the extra planning time.
Wuxi AppTec Medical device testing